Baseline patient characteristics
This study included a total of 3269 patients. Table 1 shows the baseline characteristics of participants at 30-day and 1-year follow-up. In this cohort, patients in the 30-day non-prevalence group were significantly older, with significantly greater incidence of CKD and IHD compared to the 30-day survival group. In terms of laboratory indicators, compared to the 30-day survival group, the 30-day non-prevalence group showed significantly higher levels of HGI, BUN, CR, and FBG, significantly higher WBC counts, and significantly lower LDL-C and HB levels. A similar trend was observed in 1-year follow-up results. Specifically, patients in the non-study group for one year were older than those in the surviving group. The incidence of CKD, IHD, and COPD in the Nonsurvival group was significantly greater than that in the survival group, whereas the prevalence of HTN was significantly lower than that in the survival group. Regarding laboratory indicators, compared to the survival group, the non-usurvival group once again had significantly lower HGI, significantly higher levels of BUN, CR, and FBG, significantly lower WBC counts, and significantly lower LDL-C and HB levels.
Key results of logistic regression analysis
Analysis of factors related to 30-day mortality rate
Univariate multivariate logistic regression analysis (Table 2) revealed age (univariate: OR = 1.06, 95% CI: 1.05–1.07, p <0.001; multivariate: OR = 1.05, 95% CI: 1.04–1.07, p <0.001). 0.57, 95% CI: 0.46–0.71, p <0.001: OR = 0.44, 95% CI: 0.34–0.57, p <0.001)
Lasso's regression analysis confirmed that age, HGI, HB levels, WBC counts, and BUN levels were significant predictors of mortality at 30 days and 1 year. A multivariable logistic regression model was then constructed, and the results revealed that age (OR = 1.05, 95% CI: 1.04–1.06, p <0.001) was positively correlated with 30-day mortality.
Analysis of factors related to 1-year mortality rate
We revealed that age (univariate: OR=1.06, 95% CI: 1.05–1.07, p <0.001; multivariate: OR=1.07, 95% CI: 1.06–1.08, p <0.001) was correlated for she high over the course of 1 year. 95% CI: 0.67–0.92, p = 0.003:OR = 0.69, 95% CI: 0.56–0.84, p < 0.001) was negatively correlated with 1-year mortality.
Lassologistic regression analysis confirmed that age (OR = 1.07, 95% CI: 1.06–1.07, p < 0.001) and presence of COPD (OR = 1.46, 95% CI: 1.09–1.96, p = 0.011) died 1 year and 1 year. p = 0.001) was negatively correlated with 1-year mortality.
The relationship between stratified analysis of HGI and the risk of death
To further investigate the association between HGI and the risk of death, HGI was subjected to stratified analysis by quartile (Q1-Q4) (Table 3). In Model 1, there was no adjustment for covariates. In Model 2, the models were adjusted to suit their age. In Model 3, the models were adjusted for age, HB level, WBC count, and BUN level. The risk of death over 30 days was significantly reduced compared to the Q1 group (-0.55–0.33), Q3 (0.09-0.27) and Q4 groups (0.27-2.13). [Q3 group, OR = 0.53 (95% CI: 0.38–0.73, P < 0.001) in Model 1, OR = 0.40 (95% CI: 0.29–0.56, P < 0.001) in Model 2 with the variable adjustment, and OR = 0.50 (95% CI: 0.35–0.71, P < 0.001) in Model 3; Q4 group, OR = 0.60 (95% CI: 0.44–0.82, P = 0.002) in Model 1, OR = 0.47 (95% CI: 0.34–0.65, P < 0.001) in Model 2, and OR = 0.51 (95% CI: 0.36–0.71, P < 0.001) in Model 3]. Trend testing revealed that increased HGI (i.e. from Q1 group to Q4 group) significantly reduced the risk of death (P with trend <0.0001). A similar pattern was observed at 1 year follow-up. That is, as HGI increased (i.e., from Q1 to Q4 groups), the risk of death tended to decrease.
Results of COX regression analysis
Univariate and multivariate COX regression analyses were performed to identify prognostic indicators of mortality over 30 days and 1 year. As shown in Table 4, in the analysis of 30-day mortality, age (univariable HR = 1.05, 95% CI: 1.04–1.06, P <0.001; multivariable HR = 1.05, 95% CI: 1.04–1.06, P <0.001; <0.001) was HGI (HGI(HGI)). CI: 0.48–0.72, p <0.001; COX regression analysis revealed similar trends for 1 year of death risk. Age (univariable HR = 1.05, 95% CI: 1.05–1.06, P <0.001; multivariate: HR = 1.05, 95% CI: 1.05–1.06, P <0.001) was an independent risk factor, whereas HGI (univariable: HR = 0.79, 95% CI: 0.68–0.91: multivariate: HR = 0.63, 95% CI: 0.54–0.74, p <0.001) and HB levels (HR = 0.79, 95% CI: 0.76–0.82, p <0.001) were independent protective factors in IS patients.
After screening variables in Lasso regression analysis, age (30 days: HR = 1.05, 95% CI: 1.04–1.06, P <0.001; 1 year: HR = 1.05, 95% CI: 1.04–1.06, P <0.001) left independent risk factors for both 30 days and 1 year deaths for HG. 95% CI: 0.44–0.66, P <0.001;
Kaplan – Meier (K – M) Survival Analysis
K–M survival analysis (curves shown in Figure 3A) revealed that HGI was significantly associated with 30-day mortality rates in IS patients (log rank test, p <0.001). Survival curve analysis revealed that during the 30-day follow-up period, the risk of death in the low-HGI group was significantly greater than that in the high-HGI group. This difference in survival persisted at 1 year follow-up (log rank test, p <0.001) (Fig. 3b).

KM survival curves for age and HGI levels of 30-day mortality and 1-year mortality rates for IS patients.
Furthermore, significant differences were observed in both 30-day and 1-year survival rates between patients in the older and younger groups (log rank test, p <0.001). Specifically, survival curve analysis (Fig. 3C, D) revealed that the risk of death in the older group was significantly greater than that in the younger group.
Limited average survival time
RMST analysis was employed to assess the association between HGI and 30-day mortality and 1-year mortality in patients with IS (Figure 4). Patients were divided into high HGI groups (ARM 1) and normal HGI groups (ARM 0) for comparative analysis.

RMST analysis of age and HGI levels of 30-day and 1-year mortality rates in IS patients.
During the 30-day follow-up, the mean survival rate for patients in the high HGI group was 26.70 days (95% CI: 25.88–27.51), while the mean survival rate for patients in the normal HGI group was 28.17 days (95% CI: 27.95–28.40). According to RMST analysis, the difference in RMST between the two groups was -1. 48 days (95% CI: -2.32—-0.63, p = 0.001). This was a significantly shorter survival rate for patients in the HigHI group than for patients in the normal HGI group.
This difference in survival was significant during the one-year follow-up. The mean survival rate for the high HGI group was 272.75 days (95% CI: 257.49–288.02), while the survival rate for the normal HGI group was 309.94 days (95% CI: 305.55–314.32).
Nonlinear analysis
To further explore the association between HGI and outcomes in patients with IS, RCS analysis was used to assess the nonlinear association between HGI and patient 30-day and 1-year mortality (Fig. 5).

RCS analysis of HGI levels of 30-day and 1-year mortality rates in IS patients.
RCS analysis revealed a nonlinear relationship between HGI and both the 30-day and 1-year death risk. Low HGI values were associated with a significantly increased risk of death, but as HGI increased the risk of death gradually decreased.
A significant nonlinear relationship was observed between age and risk of death in patients with IS (Figure 6). RCS predictive plots revealed that increased age significantly increased the risk of death over 30 days, with a large growth rate observed in older groups (>80 years). The association between age and risk of death was also significant in one-year mortality analysis.

RCS analysis of age of 30-day and 1-year mortality rates in IS patients.
Mediated effects of HGI on age and mortality patients with IS
Mediation analyses were performed to assess the mediated effects of HGI on the relationship between 30-day and 1-year mortality in patients with IS (Figure 7). To increase the interpretability of assessment of mediation effects, the age variable was divided by 10. As shown in Table 5 and Figure 8, the analysis of 30-day mortality rates showed that the total effect of age on mortality was 0.0017 (95% CI: 0.0010 to 0.0029, P <0.001), indicating an increased risk of death over 30 days. The mean direct effect (ADE) was 0.0019 (95% CI: 0.0010–0.0032, p <0.001), whereas the mean causal mediated effect (ACME) via HGI was -0.0001 (95% CI: −0.0003–0.0001, p <0.001). The rate of mediation for HGI was -0.0805 (95% CI: -0.1276— -0.0494, p <0.001). Negative indications indicate that as an intermediary variable, HGI has a suppressive effect on the positive relationship between age and mortality. Similar results were observed in one-year mortality assessments, indicating that the inhibitory effect of HGI remains significant in assessing long-term mortality risk.

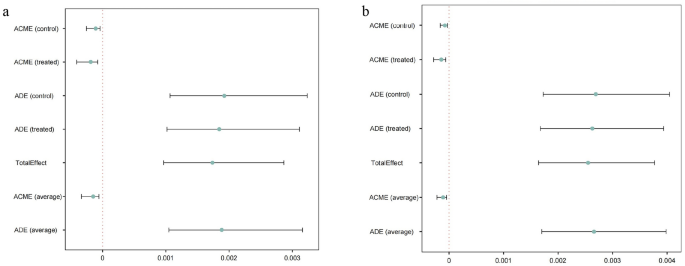
Mediates the effects of HGI on age (per 10-year increase) and mortality rates in IS patients.
Establishing and verifying predictive models
Multiple ML algorithms including SVM, XGB, RF and DT algorithms were used to construct a model predicting 30-day mortality rate in IS patients. The model was evaluated via ROC curve analysis and DCA.
In ROC curve analysis, all four ML models achieved good predictive performance. As shown in Figure 9, the AUC values differ to some extent across the model, with the RF and SVM models showing the highest accuracy of 76.66% and 76.76%, respectively.

ROC curves for four models.
Additional performance metrics for the four models are shown in Table 6. Among them, the RF model outperforms the other models in terms of recall (0.437) and F1 score (0.469), achieving the best G-Mean (0.616), identifying both positive and negative classes, suggesting that it provides a more robust classification performance.
The SHAP method was employed to explain the contribution of each feature to the performance of the ML model. As shown in Figure 10, age was the most important feature for predicting 30-day mortality rates in IS patients, followed by BUN levels, HB levels, WBC counts, and HGI.

Results of SHAP analysis.
The SHAP double sequence graph and histogram clearly show the ranking of the relative importance of each function, with age having the most important effect. The Shap Ripple plot further revealed the direction and magnitude of the effect of feature changes on predicted results, indicating that age was positively correlated with the risk of death.
A detailed analysis of the characteristic screening table and SHAP outcome matrix showed that age factors had the highest SHAP value for predicting mortality (average approximately 0.0319), indicating that age contributed the most to the prediction of the model. Although HGI was not the most important predictor, it was complementary value in the performance of the predictive model as it interacted with age, HB level and other factors.